Are there network differences between the ipsilateral and contralateral hemispheres of pain in patients with episodic migraine without aura?
Article information

Abstract
Background
We aimed to identify any differences in the structural covariance network based on structural volume and those in the functional network based on cerebral blood flow between the ipsilateral and contralateral hemispheres of pain in patients with episodic migraine without aura.
Methods
We prospectively enrolled 27 patients with migraine without aura, all of whom had unilateral migraine pain. We defined the ipsilateral hemisphere as the side of migraine pain. We measured structural volumes on three-dimensional T1-weighted images and cerebral blood flow using arterial spin labeling magnetic resonance imaging. We then analyzed the structural covariance network based on structural volume and the functional network based on cerebral blood flow using graph theory.
Results
There were no significant differences in structural volume or cerebral blood flow between the ipsilateral and contralateral hemispheres. However, there were significant differences between the hemispheres in the structural covariance network and the functional network. In the structural covariance network, the betweenness centrality of the thalamus was lower in the ipsilateral hemisphere than in the contralateral hemisphere. In the functional network, the betweenness centrality of the anterior cingulate and paracingulate gyrus was lower in the ipsilateral hemisphere than in the contralateral hemisphere, while that of the opercular part of the inferior frontal gyrus was higher in the former hemisphere.
Conclusions
The present findings indicate that there are significant differences in the structural covariance network and the functional network between the ipsilateral and contralateral hemispheres of pain in patients with episodic migraine without aura.
INTRODUCTION
Migraine is a common disabling neurological disorder with a 1-year prevalence of approximately 12%, with the cumulative incidence by the age of 85 years reaching approximately 18.5% in males and 44.0% in females.1 Migraine pain is unilateral in 60.0% of patients and bilateral in 40.0%. Furthermore, 15.1% of patients without migraine aura and 16.9% of those with migraine aura report strictly unilateral headaches without side shifting, which are called “side-locked” headaches.2
Advancements in neuroimaging over the past decade have improved our understanding of the biology of migraine, and it is now widely accepted that migraine is a complex disorder of the brain network.3,4 Functional magnetic resonance imaging (MRI) studies have consistently demonstrated that patients with migraine exhibit alterations in functional connectivity involving several areas of brain when compared with healthy controls.5 The topological organization of cortical networks is not optimal in patients with migraine.5 Migraine has also been associated with atypical brain activations in response to painful, olfactory, and visual stimuli, with significant correlations between the extent of functional abnormalities and headache frequency.4 Effective connectivity analysis based on electroencephalography demonstrates that patients with migraine show increased information transfer toward the frontocentral regions during visual stimulation, indicating copious information exchange.6 A magnetoencephalography study found that patients with migraine also show aberrantly increased connections between the sensory cortex and the frontal lobe.7 In addition, there is accumulating evidence that the structure of the gray matter is altered in patients with migraine. One meta-analysis found that patients with migraine exhibit concordant decreases in gray-matter volume in the bilateral inferior frontal gyri, right precentral gyrus, left middle frontal gyrus, and left cingulate gyrus relative to healthy controls.8 Moreover, decreases in gray-matter volume in the right claustrum, left cingulate gyrus, right anterior cingulate, amygdala, and left parahippocampal gyrus are related to the estimated frequency of headache attacks.8 One study used structural covariance network analysis based on structural volume and thickness to reveal that patients with migraine exhibit weaker structural covariance of hypothalamic regions with frontal and temporal areas relative to healthy controls.9 However, no previous studies have investigated differences in the structural covariance network between the ipsilateral and contralateral hemispheres of pain in patients with migraine.
Arterial spin labeling (ASL) is a noninvasive perfusion method that quantitatively measures cerebral blood flow in specific areas of brain tissue.10,11 Several studies have utilized ASL perfusion MRI to demonstrate that abnormal cerebral perfusion is associated with migraine headache.12 In addition, ASL perfusion MRI can measure resting brain function directly at the voxel level by magnetically labeling arterial blood using an endogenous diffusible tracer for measuring the regional cerebral blood flow, which is thought to be coupled to regional neural activity.10,11 ASL perfusion MRI can also reduce coherent noise fluctuations by combining background suppression and time-interleaved subtraction to effectively remove large nonfunctional background signals.10,11 Although most functional studies rely on blood-oxygen-level-dependent (BOLD) functional MRI, BOLD signals are affected by significant variations in the cerebral blood flow and volume and also the cerebral metabolic rate of oxygen consumption.13 Therefore, a functional network based on BOLD MRI may exhibit instability over time due to the presence of artifacts.13 To overcome these limitations and achieve more-direct measurements of brain metabolism, the novel ASL functional technique has been increasingly adopted to evaluate brain networks. Studies have measured ASL-based connectivity in healthy controls14 and in patients with various neurological disorders, including epilepsy.15,16 However, no previous studies have investigated the functional network based on cerebral blood flow determined using ASL perfusion MRI in patients with migraine.
Therefore, in this study we investigated differences in the structural covariance network based on structural volume and those in the functional network based on ASL perfusion MRI measurements of cerebral blood flow between the ipsilateral and contralateral hemispheres of pain in patients with migraine. We hypothesized that there are significant differences in the structural and/or functional networks between the two hemispheres.
MATERIALS AND METHODS
Participants
This study was approved by the Institutional Review Board of Haeundae Paik Hospital and had a cross-sectional design. We prospectively enrolled patients at a tertiary hospital based on the following criteria: 1) visited the Department of Neurology, Haeundae Paik Hospital from August 2018 to July 2020; 2) newly diagnosed with episodic migraine without aura at Haeundae Paik Hospital based on the International Classification of Headache Disorders,17 with a drug-naïve state for preventive medications; 3) unilateral migraine pain always occurring on the same side; 4) normal brain MRI findings in fluid-attenuated inversion-recovery (FLAIR) imaging and T2-weighted imaging based on visual inspections; and 5) no history of any other medical, neurological, or psychiatric disease. Written informed consent was obtained from all of the participants. We defined the ipsilateral hemisphere as the side of migraine pain.
MRI data acquisition
All MRI scans were performed using the same 3.0-T MRI scanner (AchievaTx, Phillips Healthcare, Best, Netherlands) equipped with a 32-channel head coil. The same brain MRI protocol was applied to all patients with migraine, which included three-dimensional (3D) FLAIR imaging, coronal T2-weighted imaging, 3D T1-weighted imaging, and ASL. FLAIR and T2-weighted imaging were used to evaluate structural abnormalities in the brain. All patients were in the interictal state of headache (i.e., no migraine attack) at the time of MRI scanning.
The 3D T1-weighted images were acquired using a turbofield echo sequence with the following parameters: inversion time = 1,300 ms, repetition time (TR)/echo time (TE) = 8.6 ms/3.96 ms, flip angle = 8°, and an isotropic voxel volume of 1 mm3. ASL perfusion MRI scans were acquired using a pseudocontinuous ASL (pCASL) technique and a 3D gradient and spin-echo readout. The specific imaging parameters for the pCASL experiments were as follows: TR/TE = 4,200 ms/13 ms, field of view = 240 × 240 × 120 mm, voxel size = 3 × 3 × 6 mm (20 partitions), and a parallel imaging a parallel imaging factor of 1.2.3. Dynamic scans consisting of pairs of control and magnetically labeled images were acquired using a labeling duration of 1,650 ms, a postlabeling delay of 1,800 ms, and a total scan duration of 3 minutes and 46 seconds.
MRI processing to measure structural volumes and cerebral blood flow
The structural volume was measured using the recon-all function in the FreeSurfer program. The FreeSurfer processing stream consisted of the following stages: volume registration with the Talairach atlas, bias-field correction, initial volumetric labeling, nonlinear alignment to the Talairach space, and final labeling of the volume. The cortical surface of each hemisphere was then inflated to an average spherical surface to locate both the pial surface and the boundary between white matter and gray matter. We calculated the volumes of the cortical regions of interest (ROIs) and subcortical structures including the amygdala, caudate, hippocampus, pallidum, putamen, and thalamus in the Desikan atlas (Supplementary Table 1). We then normalized the structural volume to the total intracranial volume using the following equation: structural volume (%) = (absolute structural volume)/(total intracranial volume) × 100.
Cerebral blood flow was measured using three programs based on MATLAB (Version R2020a, MathWorks, Natick, MA, USA), SPM12 (https://www.fil.ion.ucl.ac.kr/spm/), and the ASLtbx tool box (https://www.cfn.upenn.edu/~zewang/ASLtbx.php).18 We calculated the cerebral blood flow of the ROI according to the automated anatomical labeling (AAL) atlas19 (Supplementary Table 2) as follows: motion correction of ASL, registration with T1-weighted imaging, smoothing, exclusion of brain voxels, measurement of mean cerebral blood flow, normalization, and extraction of cerebral blood flow for each region. We excluded the vermis ROI in the AAL atlas because it could not be classified into right and left sides.
Network analysis using graph theory
We analyzed the structural covariance network based on structural volume and the functional network based on cerebral blood flow using BRAPH software (http://braph.org/).20 To combine patients with right- and left-sided migraine pain into a single cohort, the regions were converted from the right or left side to the ipsilateral or contralateral side according to the side of migraine pain. We constructed a collection of nodes representing brain regions connected by edges corresponding to the connections between them. The nodes were defined using the structural volume or cerebral blood flow of the ROI, and the edges corresponded to the partial correlation coefficients between the pairs of brain regions while controlling for the effects of age and sex. An undirected and weighted connectivity matrix was constructed for each group. To detect differences between groups in the global network topology, we calculated the average degree, average strength, radius, diameter, eccentricity, characteristic path length, global efficiency, local efficiency, mean clustering coefficient, transitivity, modularity, assortative coefficient, and small-worldness index.20,21 To assess differences in local network topology between groups, we calculated the betweenness centrality of the ROI, which is the most commonly used measure for reflecting network centrality.20,21
Statistical analysis
A primary analysis was applied to the data using an a-priori test. No statistical power calculation was conducted prior to the study, with the sample size instead being based on the available data. Differences in structural volume and cerebral blood flow between groups were analyzed using independent-samples t-tests. We used a histogram to visually determine whether the data were sufficiently symmetric to apply t-tests. Comparisons of the structural covariance network and the functional network were performed using nonparametric permutation tests with 1,000 permutations, with the network measures obtained at the group level. The tests were performed by first randomly permuting the subjects from both groups and then calculating the differences in the graph measures between the new randomized groups. This procedure was repeated 1,000 times to obtain the distribution of between-group differences. The p-values were then calculated as the fractions of the difference distribution values that exceeded the difference values between the actual groups.
Categorical variables are presented as frequencies and percentages, and continuous variables are presented as mean ± standard deviation or median and interquartile-range values. Statistical significance was set at a twotailed p-value of <0.05. False-discovery-rate correction for multiple comparisons was applied when analyzing the structural covariance network and the functional network. MedCalc® statistical software (version 19.6; MedCalc Software, Ostend, Belgium; https://www.medcalc.org) was used for the statistical analysis.
RESULTS
Participants
Twenty-eight patients with newly diagnosed migraine with unilateral pain underwent brain MRI scanning. Visual inspections of brain MRI scans revealed structural lesions in one of these patients, who was then excluded from the study. Thus, we finally enrolled 27 patients with migraine without aura. There were no missing data for these patients. Table 1 lists the clinical characteristics of the patients, whose mean age was 41.5 years and included four males. Fifteen patients experienced right-sided migraine pain, while the other 12 experienced left-sided migraine pain.
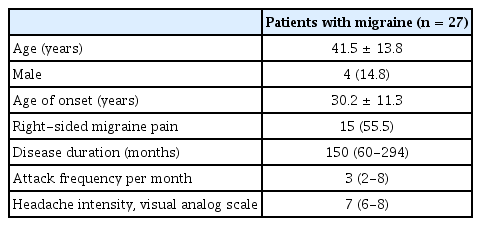
Clinical characteristics of patients with migraine
Structural volume and cerebral blood flow
There were no significant differences in the structural volumes (Supplementary Table 1) or cerebral blood flows (Supplementary Table 2) of the ROIs between the ipsilateral and contralateral hemispheres.
Structural covariance network based on structural volume
None of the parameters of the global structural covariance network differed significantly between the ipsilateral and contralateral hemispheres (Table 2). However, there were significant differences in the local structural covariance network, with the betweenness centrality of the thalamus being significantly lower in the ipsilateral hemisphere than in the contralateral hemisphere (0.000 vs. 0.162, p = 0.027) (Table 3, Fig. 1, Supplementary Table 3).
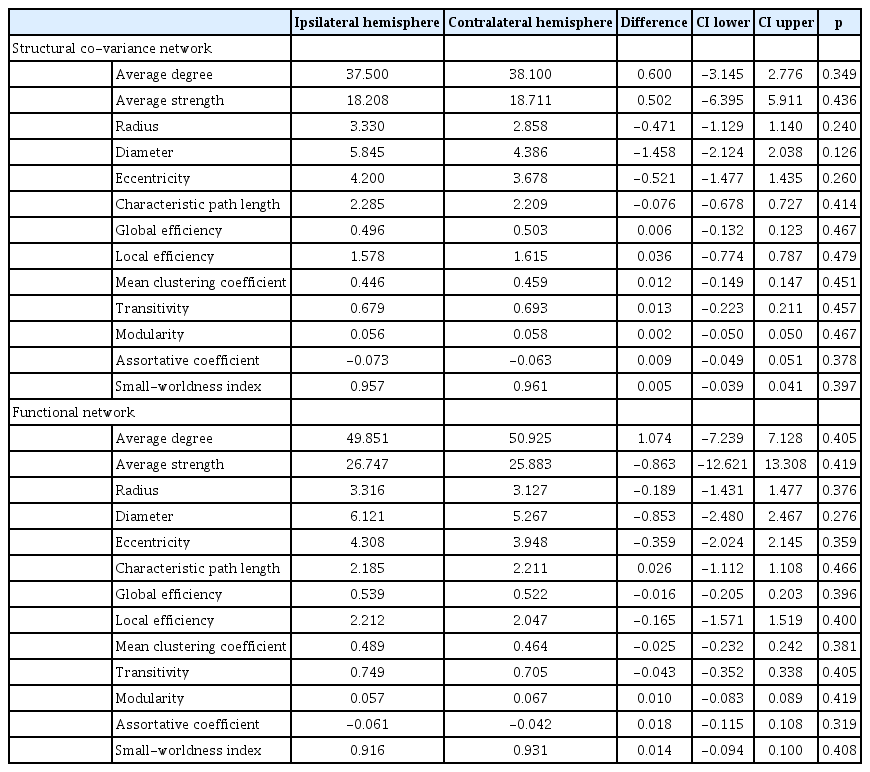
Differences in the global structural covariance network based on structural volume and the functional network based on cerebral blood flow between the ipsilateral and contralateral hemispheres of pain in patients with migraine

Regions with significant differences in the local structural covariance network based on structural volume and the functional network based on cerebral blood flow between the ipsilateral and contralateral hemispheres of pain in patients with migraine
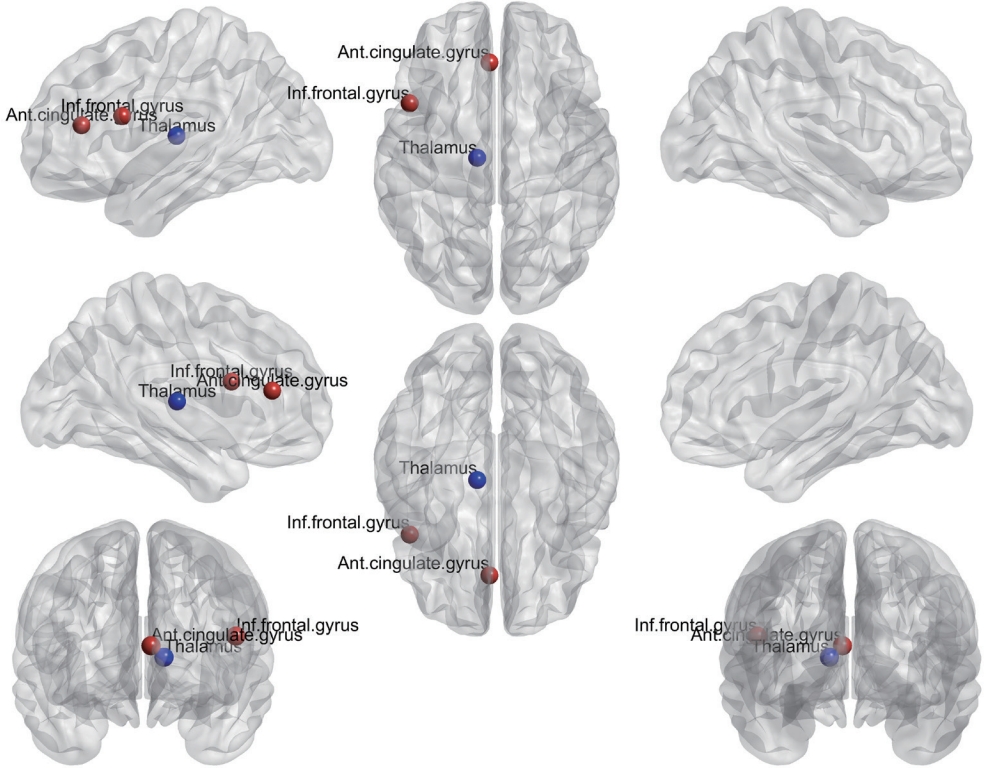
Regions with significant differences in the local structural covariance network based on structural volume (blue circles) and the functional network based on cerebral blood flow (red circles) between the ipsilateral and contralateral hemispheres of pain in patients with migraine.
Functional network based on cerebral blood flow
None of the parameters of the global functional network differed significantly between the ipsilateral and contralateral hemispheres (Table 2). However, there were significant differences in the local functional network, with the betweenness centrality of the anterior cingulate and paracingulate gyrus being significantly lower and that of the opercular part of the inferior frontal gyrus being significantly higher in the ipsilateral hemisphere than in the contralateral hemisphere (0.000 vs. 0.261, p = 0.038; 0.018 vs. 0.000, p = 0.019; respectively) (Table 3, Fig. 1, Supplementary Table 4).
DISCUSSION
This study investigated differences in the structural covariance network and the functional network between the ipsilateral and contralateral hemispheres of pain in patients with migraine. Our results indicated that the structural volume and cerebral blood flow did not differ significantly between the ipsilateral and contralateral hemispheres. However, significant differences in the structural covariance network and the functional network were observed between the two hemispheres. In addition, we have demonstrated the feasibility of functional network analysis using ASL perfusion MRI in patients with migraine.
We found that, in the structural covariance network, the betweenness centrality of the thalamus was significantly lower in the ipsilateral hemisphere than in the contralateral hemisphere. Alterations in the structural covariance network may reflect alterations in dendritic complexity, changes in the number of synapses, or brain plasticity that result in connectivity changes.22 Betweenness centrality is a measure of centrality in a graph based on the shortest paths, which is a widely used measure to detect the amount of influence that a node has over the flow of information in a graph.23 This measure quantifies the number of times that a node acts as a bridge along the shortest path between two other nodes.23 Thus, the present findings suggest that the structural connectivity of the thalamus is lower in the ipsilateral hemisphere than in the contralateral hemisphere during the interictal state. In the pathogenesis of migraine, the thalamus may play a role as a relay center for ascending nociceptive information from the brainstem to cortical regions via the trigeminovascular pain pathway.24 The thalamus is therefore most likely involved in the allodynia, central sensitization, and photophobia associated with migraine.24 Previous studies using functional MRI25 and diffusion-tensor imaging26 have also observed abnormal thalamocortical network connectivity in patients with migraine. In addition, we recently demonstrated that thalamic nuclei volumes differ significantly between patients with migraine and healthy controls, especially in the anteroventral, medial geniculate, and parafascicular nuclei.27 Together these findings suggest that alterations in thalamic connectivity contribute to the pathogenesis of migraine.
Our functional network analysis based on cerebral blood flow revealed significant alterations in the betweenness centrality of the anterior cingulate and paracingulate gyrus. The cingulate gyrus is involved in pain processing, modulation, and associated symptoms such as emotional disturbances in patients with migraine.8 Previous functional MRI studies have consistently found atypical brain responses to sensory stimuli, absence of the normal habituating response between attacks, and atypical functional connectivity of sensory processing regions in patients with migraine.4 The alterations in the betweenness centrality of the cingulate gyrus revealed by our functional network analysis are consistent with previous findings, supporting the notion that sensory hypersensitivities in patients with migraine may be induced by a combination of enhanced sensory facilitation and reduced inhibition in response to sensory stimuli.28,29 Furthermore, the cingulate gyrus is one of the regions of the default-mode network (DMN) that plays a role in adaptive behaviors other than those associated with cognitive, emotional, and attentional processes.30 Several studies have identified disruption of DMN connectivity during the interictal period in patients with migraine.31 Pain has a widespread impact on overall brain function by modifying brain dynamics beyond only pain perception, which may induce alterations in DMN connectivity.32 Based on the amplitude of low-frequency fluctuations, another functional MRI study found reduced DMN connectivity in the anterior cingulate cortex, prefrontal cortex, and thalamus in patients with migraine.33 Furthermore, functional DMN changes are negatively correlated with disease duration.33 Together these observations indicate that the cingulate gyrus may be involved in pain processing in patients with episodic migraine without aura.
In this study we also observed that the betweenness centrality of the inferior frontal gyrus was higher in the ipsilateral hemisphere than in the contralateral hemisphere. The frontal cortex is one of the most important areas associated with brain abnormalities in patients with migraine. The role of the frontal lobe in pain processing has been established in previous studies, including those involving patients with chronic back pain, fibromyalgia, phantom pain syndrome, and medication-overuse headache.34 A previous meta-analysis found that patients with migraine exhibited concordant decreases in gray-matter volume in the inferior frontal gyrus.8 Increased activation in the inferior frontal gyrus may reflect increased effort due to disorganization of these areas or the use of compensatory strategies involving pain processing in migraine.8 Additionally, one functional MRI study found that the increased neural activation in the frontal gyrus in response to fearful faces relative to neutral faces was greater in patients with migraine than in healthy controls. Thus, an enhanced response to emotional stimuli may explain the triggering effect of psychosocial stressors on episodic migraine without aura.35
In addition to migraine, several previous studies have demonstrated that the betweenness centrality of the brain can change in various other diseases related to pain, such as fibromyalgia, post-coronavirus disease pain, disc herniation, and knee osteoarthritis.36-39 These are consistent with our present findings.
In this study we found no volume or perfusion differences between the hemispheres, but the covariance network analysis did identify differences, which indicates a change in the connection between nodes rather than a specific abnormality in each region, and thus provides evidence that migraine is a network disease. A covariance network analysis can identify which nodes have the greatest influence on other nodes, thereby revealing key hubs in the complex brain system.40 Such an analysis can help reduce the dimensionality of high-dimensional data by graphically summarizing the relationships between variables. This may improve computational efficiency and simplify data interpretation. In addition, covariance network analysis can be extended to investigate dynamic networks to capture how the relationships between variables change over time.40
This is the first study to investigate differences in the structural and functional networks between the hemispheres according to the side of migraine. We found significant differences in the structural and functional networks of some regions between the ipsilateral and contralateral hemispheres. Furthermore, our findings highlight the feasibility of functional network analysis based on cerebral blood flow determined using ASL in patients with migraine. However, this study had several limitations. First, the sample was relatively small, which was due to us only enrolling patients who had unilateral migraine pain that always occurred on the same side. In addition, all patients were newly diagnosed with migraine without aura and underwent MRI during the interictal state. Second, we did not perform ASL perfusion MRI on healthy controls, and so we could not investigate differences in the structural and functional networks between patients with migraine and healthy controls. Third, we could not analyze the correlation between clinical factors and network measures since we obtained network measures at the group rather than the individual level. Fourth, we did not collect certain clinical characteristics from patients with migraine, such as the family history of migraine, specific triggering factors, quality of life, or stress and anxiety scores. In addition, most patients with migraine in our study were taking medications for pain, which might have impacted their structural and/or functional networks. Fifth, we could not evaluate cerebral arterial images in participants, such as those obtained using magnetic resonance angiography. This condition could have affected the ASL images. Further studies with larger samples may be required to confirm our findings.
The present findings demonstrate that there are significant differences in the structural covariance network and the functional network between the ipsilateral and contralateral hemispheres of pain in patients with episodic migraine without aura. These findings may be related to the pathogenesis of pain in these patients.
Supplementary Material
Supplementary Materials can be found with this article online https://doi.org/10.14253/acn.2023.25.2.93
Supplementary Table 1.
Differences in structural volume between the ipsilateral and contralateral hemispheres of pain in patients with migraine
Supplementary Table 2.
Differences in cerebral blood flow between the ipsilateral and contralateral hemispheres of pain in patients with migraine
Notes
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Acknowledgements
This work was supported by the National Research Foundation of Korea NRF) grant funded by the Korea government MSIT) No. RS-2023-00209722)